FDOJ Cavitations
A jawbone alteration that can go undetected on conventional X-rays. Its possible relationship with systemic symptoms is being actively investigated.
 Healthy bone vs. FDOJ cavitation
Healthy bone vs. FDOJ cavitationImportant scientific information
Cavitations (FDOJ) are a recognized morphological entity with documented histological evidence. However, the relationship between FDOJ and systemic symptoms (fatigue, autoimmunity, etc.) is still under investigation. There are currently no randomized controlled trials (RCTs) demonstrating that FDOJ treatment improves these symptoms.
What are cavitations?
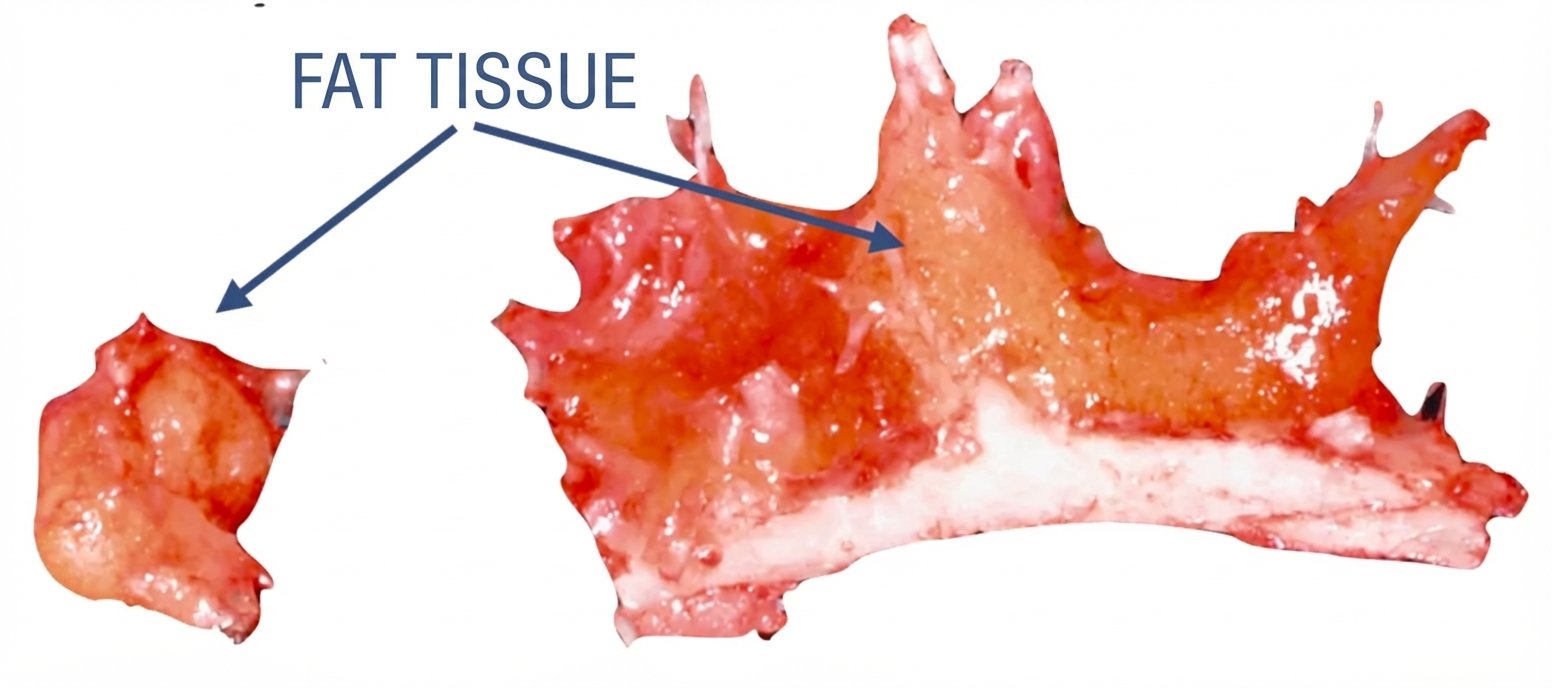
Cavitations are areas within the jawbone where tissue has not healed properly after a tooth extraction or other procedure. Instead of healthy bone, we find fatty tissue, necrotic tissue, and inflammatory mediators.
Unlike an acute infection that produces pain and pus, cavitations are a chronic, ischemic process (lack of blood supply). This is why they can go undetected for years.
RANTES/CCL5: Current research
What does science say about cavitations and systemic inflammation?
What is RANTES/CCL5?
RANTES (Regulated upon Activation, Normal T-cell Expressed and Secreted), also known as CCL5, is a pro-inflammatory chemokine. Recent studies (Lechner et al., 2021) have documented that FDOJ tissue overexpresses this protein.
Important: In the general scientific literature, elevated RANTES levels have been observed in patients with various conditions. However, the causal relationship between FDOJ and these conditions is still being investigated. It has not been proven that treating FDOJ improves these symptoms.
Conditions where elevated RANTES has been observed in general literature:
 Jawbone fragment with fatty degeneration (FDOJ)
Jawbone fragment with fatty degeneration (FDOJ)Symptoms reported in patients with FDOJ
Important clarification
Most FDOJ cavitations are completely asymptomatic and are discovered incidentally on CBCT. The following symptoms have been reported in some patients with diagnosed FDOJ, but they are not specific to this condition. If you have these symptoms, consult your doctor to rule out other causes first.
Local symptoms
When FDOJ is symptomatic
Facial neuralgia or NICO
Atypical facial pain or trigeminal neuralgia. Sometimes described as “phantom pain” in areas where there are no longer teeth.
Referred pain
Pain that radiates to the ear, neck, or head without apparent cause in those areas.
Pressure sensation
Some patients describe a subtle sensation of “hollowness” or diffuse discomfort in the jaw area.
Systemic symptoms
Reported but non-specific – consult your doctor
Chronic fatigue
Feeling of exhaustion without apparent cause. May have multiple origins – rule out other causes first.
Brain fog
Difficulty concentrating or memory problems. Common symptom in many conditions.
Rheumatic symptoms
Joint pain or inflammation. Requires complete medical evaluation before attributing to FDOJ.

Why do normal X-rays not detect them?
Cavitations are frequently invisible on 2D panoramic X-rays. The superposition of structures hides bone density loss until the damage is very extensive (more than 30-50% loss).
That is why we use Cone Beam CBCT technology (3D Tomography) for a more reliable diagnosis.
Three-dimensional vision
We evaluate the bone architecture in 3D, eliminating superpositions and distortions.
Density detection
We reveal hypodense areas (low density) that may correspond to fatty degeneration.
Surgical planning
We precisely locate the extent of the lesion to plan treatment if indicated.
Regenerative protocol
When indicated, we remove necrotic tissue and stimulate natural bone regeneration with minimally invasive surgery.
Surgical cleaning
Deep curettage to remove documented fatty and necrotic tissue until reaching healthy bone.
Ozone therapy
Ozone gas to disinfect the area and improve tissue oxygenation.
Regenerative PRF
Platelet-Rich Fibrin from your own blood to promote healing and bone regeneration.
Follow-up
Periodic monitoring to evaluate bone regeneration and the patient clinical evolution.
Remove a focus of chronic inflammation
The treatment aims to remove documented necrotic tissue. Possible systemic benefits are based on theoretical mechanism and clinical experience, not on controlled clinical trials. Response to treatment is variable and not guaranteed.
Remove necrotic tissue
We remove documented tissue with RANTES overexpression. The impact on systemic markers varies according to each patient.
Possible vitality support
Some patients report improved energy after treatment. This response is variable and not guaranteed.
Reported clinical experience
In cases of symptomatic FDOJ, some patients report cognitive improvement. Individual results may vary.
Possible local pain relief
In cases of associated facial neuralgia (NICO), treatment may help relieve pain, although each case is different.
Reduce burden on the body
Remove necrotic tissue puede reducir una carga para el sistema inmune. Beneficios sistémicos no garantizados.
Promote bone regeneration
With the PRF protocol we seek to stimulate natural bone regeneration. Results may vary according to each patient.
Frequently asked questions
FDOJ has been a recognized morphological entity since 1992 (Bouquot) with documented histological evidence. Recent studies such as Lechner et al. (2021) have demonstrated RANTES overexpression in FDOJ samples. There is legitimate scientific discussion about: (1) How to standardize CBCT diagnosis, (2) Which are clinically significant vs incidental findings, (3) Which patients truly benefit from treatment (controlled trials are lacking). At BDS we apply rigorous protocols and acknowledge these limitations in consultation.
Not necessarily. Many cavitations are asymptomatic incidental findings. The recommended protocol is: periodic CBCT follow-up, evaluation of related local or systemic symptoms, and treatment only if there are clear local symptoms (neuralgia, pain) or if the patient chooses treatment after weighing risks/benefits. The presence of FDOJ on CBCT does not mean it must be treated.
If you have had wisdom teeth or other teeth extracted, if you have root canals, or if you suffer from atypical facial pain without clear explanation, it may be worth having a diagnostic CBCT. Cavitations usually do not cause local pain, so the absence of pain does not rule them out. If you have systemic symptoms (fatigue, etc.), we recommend ruling out other causes with your doctor first.
The surgery is performed under local anesthesia and is minimally invasive. Thanks to ozone therapy and PRF, the postoperative period is usually manageable, with controllable discomfort and enhanced healing.
Bone regeneration is a gradual process that can take several months. Times vary according to each patient and the extent of the lesion. During postoperative follow-up, we evaluate progress and accompany you throughout the recovery process.
The cost depends on the number and extent of cavitations. It includes diagnostic CBCT, surgery, ozone therapy, and PRF. We will give you a personalized quote after the initial evaluation.
Rigorous diagnosis
A CBCT diagnosis can reveal hidden cavitations. We explain the options with transparency and scientific rigor.